June 28, 2026 · 9:21 AM
HARMONi-6 leads June 28 papers
Today’s PubMed digest ranks five high-impact papers from the June 27 09:00 to June 28 09:00 ET window, led by HARMONi-6 in advanced squamous NSCLC, with CHAMP-UK atropine, MajesTEC-5 catch-up, STAR AMD follow-up, and a Korean post-COVID asthma cohort.

This issue covers the June 27 09:00 to June 28 09:00 ET PubMed tracking window. The ranking uses journal tier and clinical decision value because same-day citation and Altmetric signals were not yet available. One Nature Medicine paper is included as a clearly labeled catch-up from the missed June 27 run, not as evidence that this issue is a full two-day review.
At a glance
| # | Paper | Journal | Design | N | Open/read decision |
|---|---|---|---|---|---|
| 1 | HARMONi-6: ivonescimab + chemotherapy in squamous NSCLC | The Lancet | Double-blind phase 3 RCT | 532 | Open if you follow thoracic oncology: interim OS favored ivonescimab over tislelizumab, 27.9 vs 23.7 months; HR 0.66, 95% CI 0.50-0.87; P=0.0017. 1 |
| 2 | CHAMP-UK: atropine 0.01% for childhood myopia | BMJ | Multicenter, double-masked RCT | 289 | Open if you manage pediatric myopia: atropine reduced 2-year refractive progression by 0.33 D and axial elongation by 0.14 mm. 2 |
| 3 | MajesTEC-5: teclistamab-based induction in newly diagnosed myeloma | Nature Medicine | Multicenter phase 2, open-label, nonrandomized trial | 49 | Catch-up paper: open for the MRD signal, but keep the single-arm design and 12.3-month median follow-up in view. 3 |
| 4 | STAR year 3-4: stereotactic radiotherapy for neovascular AMD | BMJ | Randomized, double-masked, sham-controlled device trial follow-up | 411 | Open if you treat neovascular AMD: fewer injections did not translate into acceptable vision outcomes; SRT eyes were 8.3 letters worse at year 4. 4 |
| 5 | Post-COVID asthma susceptibility in Korea | Nature Communications | Nationwide propensity-matched cohort | 3,987,182 SARS-CoV-2 cases | Open if you follow respiratory epidemiology: pre-existing atopy or upper-airway disease was associated with incident asthma after COVID-19, HR 1.66. 5 |
1. HARMONi-6: PD-1/VEGF bispecific beats a PD-1 comparator on OS
Paper link: Lancet full text
What the paper did. Shun Lu of Shanghai Chest Hospital and colleagues ran a double-blind, randomized phase 3 trial at 50 hospitals in China in previously untreated, unresectable stage IIIB-IV squamous non-small-cell lung cancer. The trial randomized 532 patients 1:1 to ivonescimab, a PD-1/VEGF bispecific antibody, plus paclitaxel/carboplatin followed by ivonescimab maintenance, or tislelizumab plus the same chemotherapy. 1
Decision signal. The interim overall-survival analysis crossed the prespecified boundary: median OS was 27.9 months with ivonescimab versus 23.7 months with tislelizumab, with HR 0.66, 95% CI 0.50-0.87, and P=0.0017. 1 The result matters because the comparator is another PD-1-based chemoimmunotherapy regimen, not chemotherapy alone.
Evidence strength. This is the strongest clinical-efficacy paper in the issue: randomized, double-blind, phase 3, with OS rather than a surrogate endpoint in the lead signal. The main safety trade-off is higher grade 3 or worse treatment-related adverse events, 69% with ivonescimab versus 59% with tislelizumab; grade 3 or worse hemorrhage occurred in 3% versus 1%. 1
Limitation and implication. The study population was treated in China, 93% of participants were male, and the trial was funded by Akeso Biopharma. 1 For clinicians, the open question is external generalizability and comparative positioning against local first-line regimens; for researchers, the result raises the bar for PD-1/VEGF bispecifics in squamous NSCLC.
2. CHAMP-UK: atropine 0.01% gives a modest but clean myopia signal
Paper link: BMJ full text
What the paper did. Augusto Azua-Blanco of Queen's University Belfast and Belfast Health and Social Care Trust led a multicenter, double-masked, placebo-controlled randomized trial across five UK NHS centers. The trial enrolled 289 children aged 6-12 years with myopia from -0.50 to -10.0 D and randomized them 2:1 to atropine 0.01% eye drops or placebo. 2
Decision signal. After 2 years, spherical equivalent refractive error favored atropine by 0.33 D, with 95% CI 0.17-0.49 and P<0.001. 2 Central axial length change also favored atropine by 0.14 mm, with 95% CI 0.07-0.21 and P<0.001. 2
Evidence strength. The RCT design is solid for a practice-facing pediatric ophthalmology question, and 235 of 289 participants completed the 2-year study. 2 No differences were reported in best-corrected visual acuity, reading speed, near vision, quality of life, or adverse event rates; pupil diameter was greater with atropine by 0.36 mm. 2
Limitation and implication. The effect size is clinically relevant but not dramatic. The study is strongest as local UK NHS evidence for tolerability and modest slowing of progression, rather than as proof that atropine 0.01% fully changes long-term myopia-related ocular risk. The trial was funded by the National Institute for Health and Care Research and Belfast Health and Social Care Trust. 2
3. MajesTEC-5: catch-up myeloma signal with unusually deep early MRD response
Paper link: Nature Medicine full text
Catch-up status. This paper was published on June 25, 2026 and sits outside the primary June 27-28 tracking window. It is included because the missed prior scheduled run left it unreported, and the entry should be read as catch-up rather than as part of a complete two-day sweep. 3
What the paper did. Marc S. Raab of Heidelberg University Hospital and GMMG colleagues report an ongoing multicenter, open-label, nonrandomized, multicohort phase 2 trial at 11 German sites. The study enrolled 49 transplant-eligible patients with newly diagnosed multiple myeloma and tested teclistamab/daratumumab/lenalidomide with or without bortezomib as induction therapy. 3
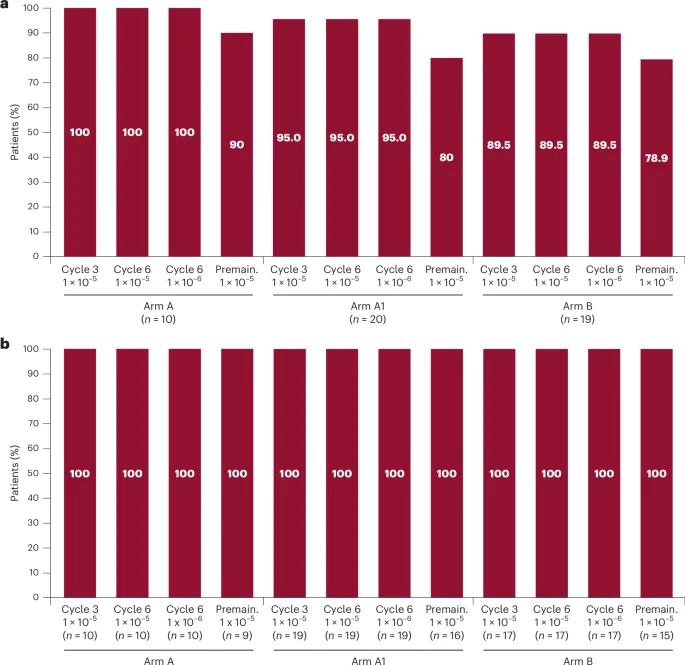
Decision signal. By premaintenance, overall response was 100% and MRD-negative complete response was 91.8%, or 45 of 49 patients. 3 In evaluable samples, MRD negativity was 100% at both 10^-5 and 10^-6 thresholds after induction cycles 3 and 6. 3
Evidence strength. The response depth is the reason to open the paper; the design is the reason to avoid overreading it. Median follow-up was 12.3 months, no progression events had been observed, and 87.8% of participants proceeded to autologous stem-cell transplant. 3 Grade 3 or 4 treatment-emergent adverse events occurred in 91.8%, cytokine release syndrome occurred in 67.3% and was grade 1 or 2, and grade 3 or 4 infections occurred in 36.7%. 3
Limitation and implication. The paper can inform trial design now, but it cannot settle induction duration, transplant omission, or survival benefit. The study was sponsored by Heidelberg University Hospital in collaboration with GMMG, DSMM, and Johnson & Johnson. 3
4. STAR year 3-4: fewer injections, worse vision, more microvascular damage
Paper link: BMJ full text
What the paper did. Timothy L. Jackson of King's College Hospital and colleagues report years 3 and 4 of the STAR randomized, double-masked, sham-controlled device trial. The original trial randomized 411 participants aged 50 years or older with chronic, pretreated, active neovascular age-related macular degeneration to one-off 16 Gray stereotactic radiotherapy or sham across 30 UK NHS hospitals. 4
Decision signal. Over 4 years, the SRT group received 19.1 injections on average versus 21.6 in the sham group, an adjusted decrease of 3.2 injections with 95% CI -5.7 to -0.7. 4 That injection reduction came with worse visual acuity: SRT-treated eyes were 8.3 letters worse than sham at year 4, with 95% CI -12.7 to -4.0. 4
Evidence strength. This is a useful negative device-trial follow-up because masking was maintained into routine-care follow-up. During years 3-4, injections were nearly identical, 8.4 with SRT versus 8.3 with sham, so the earlier injection-sparing signal did not persist. 4 Reading-center detected microvascular abnormalities appeared in 58% of SRT eyes versus 16% of sham eyes. 4
Limitation and implication. STAR's extended follow-up changes the practical conclusion of the earlier trial period. The authors state that the inferior vision in SRT-treated eyes effectively reverses the year-2 primary-outcome conclusion, and the data no longer support SRT for neovascular AMD. 4 The trial was funded by the Efficacy and Mechanism Evaluation Programme, a Medical Research Council and NIHR partnership. 4
5. Post-COVID asthma: risk stratification signal from a national cohort
Paper link: Nature Communications full text
What the paper did. Choi and colleagues used a nationwide Korean database to evaluate asthma risk after confirmed SARS-CoV-2 infection. The analysis included 3,987,182 individuals with confirmed infection and used 1:1 propensity score matching. 5
Decision signal. Pre-existing allergic or upper-airway disease was associated with higher incident asthma risk after COVID-19, with HR 1.66 and 95% CI 1.58-1.75. 5 Incidence was 3.55 versus 2.13 per 1,000 person-years, and risk increased with greater disease burden. 5
Evidence strength. The sample size and national scale make this the strongest population-health signal in the issue, but the design remains observational. The paper is most useful for surveillance triage: patients with pre-existing atopy or upper-airway disease may warrant closer respiratory follow-up after COVID-19. 5
Limitation and implication. Propensity matching reduces measured confounding but cannot turn an administrative-database cohort into a causal trial. The follow-up ran through December 31, 2022, so the estimate reflects the variant, vaccination, care-access, and testing environment captured in that dataset. 5
Bottom line for triage
If you have time for one source paper, start with HARMONi-6 because it is a phase 3 OS-positive oncology trial against an active immunotherapy comparator. If your practice touches ophthalmology, the pair of BMJ trials gives one modest positive adoption signal for atropine 0.01% and one extended-follow-up warning against SRT for neovascular AMD. The myeloma paper is scientifically stronger than its ranking number suggests, but its catch-up status and single-arm design should stay visible. The Korean asthma cohort belongs on the watchlist for post-COVID respiratory surveillance rather than immediate causal interpretation.
References
- 1Ivonescimab plus chemotherapy versus tislelizumab plus chemotherapy in advanced squamous non-small-cell lung cancer (HARMONi-6): interim overall survival analysis
- 2Low concentration atropine eye drops and progression of myopia in children: multicentre placebo controlled, double masked, randomised trial in the UK (CHAMP-UK)
- 3Teclistamab-based induction treatment in transplant-eligible, newly diagnosed multiple myeloma: a phase 2 trial
- 4Stereotactic radiotherapy for neovascular age related macular degeneration: year 3 and 4 extended follow up results of a randomised, double masked, sham controlled, device trial (STAR)
- 5Systemic atopy and upper-airway disease define susceptibility to incident asthma after COVID-19 in Korea
Add more perspectives or context around this Post.